Photo from wikipedia
Dear Editor, The occurrence of both lymphoproliferative disorder and breast cancer is a rare event. While the condition of coexistence of lymphoma and breast carcinoma has been described in the… Click to show full abstract
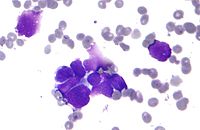
Dear Editor, The occurrence of both lymphoproliferative disorder and breast cancer is a rare event. While the condition of coexistence of lymphoma and breast carcinoma has been described in the lymph nodes [1] and in the spleen [2], no reports have been published concerning the same association in the bone. When there is a clinical suspicion that there may be a concurrence of diseases, radiological exams are carried out but the diagnosis requires histological confirmation with either biopsy or aspiration [3]. A 59-year-old woman with a previous history came under our observation for an exophytic sternal mass and right inguinal lymphadenopathy with lymphocytosis in peripheral blood (absolute lymphocyte count 7 × 10/L) according to laboratory tests. In 2001, she underwent a hysterectomy, pelvic lymphadenectomy, and radio-chemotherapy for endometrial neoplasia. In 2009, while she was in complete remission of her primary tumor, she was diagnosed with invasive ductal breast carcinoma and treated with surgical excision, radio-chemotherapy, and aromatase inhibitor. Follow-up of her breast cancer was unremarkable until September 2013 when the physical examination revealed an exophytic anterior chest wall mass, in absence of hepato-splenomegaly or other lymphadenopathies except for right inguinal lymph nodes with a diameter of 4 cm. The FDG PET-CT scan showed significant glucose hypermetabolic lesions only in the sternum, while the inguinal lymph node resulted negative. The only option to determine the nature of the disease was to perform a fine-needle aspiration from the sternal mass. The smear of the sternal aspirate documented a mixture of monomorphic medium-sized mature lymphocytes (Fig. 1A) and cohesive clusters of large cells with reticular dispersed chromatin, abundant frequently vacuolated cytoplasm (Fig. 1B), whose metastatic origin was confirmed by estrogen receptor positivity (inset in panel B). At the same time, blood and bone marrow immunophenotypic analysis showed a clonal CD19+ CD5-/CD10-/CD23lymphoid population. Lymphoproliferative disorder (marginal zone type) with concomitant breast carcinoma relapse was diagnosed. The patient received local radiotherapy and started tamoxifen. Our case is peculiar because the FDG PET/CT scan allowed to detect a single avid lesion which was in the sternum, where the only way to make the diagnosis of the two concomitant diseases was by sampling. Even if the possibilities of bone metastasis from a solid tumor were high, the diagnosis required a tissue biopsy [4, 5]. In our case, considering the site of the lesion in the sternum, fine-needle aspiration was the best option. Similarly to other cases [3], the cytological diagnosis was supported by immune histochemistry and flow cytometry. This case confirms how cytological examination of needle aspirate remains a rapid and cost-effective diagnostic tool. * Francesco Autore [email protected]
Journal Title: Annals of Hematology
Year Published: 2020
Link to full text (if available)
Share on Social Media: Sign Up to like & get
recommendations!