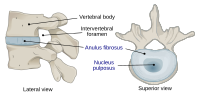
Photo from wikipedia
We analysed 100 patients following anterior cervical discectomy and fusion with interbody stabilisation with PEEK cages. Radiographs obtained preoperatively and during the 12-month follow-up were compared to track changes in… Click to show full abstract
We analysed 100 patients following anterior cervical discectomy and fusion with interbody stabilisation with PEEK cages. Radiographs obtained preoperatively and during the 12-month follow-up were compared to track changes in overall and local cervical lordosis and disk space height. Subsidence was defined as cage migration ≥ 3 mm into the adjacent endplates. Mean change in operated disk space height was 1.13 ± 1.33 mm. Subsidence was detected in 10.23% of the operated spaces. Mean change in overall cervical lordosis was 1.31 ± 5.71 degrees, and mean change in local lordosis was 0.19 ± 4.71 degrees. Change in overall cervical lordosis correlated with change in local lordosis (r = 0.61, p < 0.01). The greatest changes in lordosis and disk space height were noted immediately post-surgery. Baseline values were approximated gradually over time, but the post-operative values at 12 months were still higher than baseline. Disk space height change did not correlate with changes in patient-reported pain intensity at baseline (VAS 0) vs. at 12 months post-operatively (VAS 12) (r = 0.12, p < 0.05) or changes in the Neck Disability Index (NDI) at baseline (NDI 0) vs. at 12 months post-operatively (NDI 12) (r = -0.02, p = 0.05). Changes in overall cervical lordosis did not directly influence treatment outcomes assessed by comparing VAS 0 vs. VAS 12 (r = 0.13, p = 0.24) or NDI 0 vs. NDI 12 (r = -0.0005, p = 0.96). Surgical outcomes depend primarily on adequate decompression of the spinal cord and nerve roots. Post-operative radiological changes did not directly influence patients' pain level or quality of life.
Journal Title: Journal of Clinical Neuroscience
Year Published: 2018
Link to full text (if available)
Share on Social Media: Sign Up to like & get
recommendations!