Photo from wikipedia
A 77-year-old woman with history of anterior rectal resection for neoplasia in 1998, followed by chemoand radiotherapy, was referred to our unit because of an increase in subocclusive episodes (1–2… Click to show full abstract
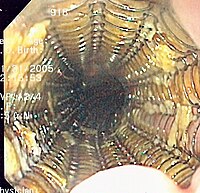
A 77-year-old woman with history of anterior rectal resection for neoplasia in 1998, followed by chemoand radiotherapy, was referred to our unit because of an increase in subocclusive episodes (1–2 times a week) over the previous 5 months, due to a stenosis extending to 5 cm above the colorectal anastomosis. The patient had previously undergone several pneumatic dilation procedures for anastomotic stenosis, with substenosis of the colon above, following radiotherapy. A computed tomography scan showed a benign stenosis of the anastomosis extending to 5 cm of the colon above, with wall thickening from the development of fibrotic tissue after radiotherapy. We performed a colonoscopy to confirm the clinical scenario; the colorectal anastomosis was located 4 cm from the anal verge (▶Fig. 1). We planned to place a modified, esophageal, large-diameter, fully covered, self-expandable metal stent (FCSEMS), with an anti-migration system and proximal head (26mm diameter, 100mm length, 34mm head; Taewoong Medical, Gyeonggi-do, South Korea). Under deep sedation, the patient underwent lower endoscopy with a gastroscope. The proximal and the distal ends of the stricture were marked with a submucosal injection of radiopaque contrast medium. A guidewire (Jagwire; Boston Scientific, Marlborough, Massachusetts, USA) was advanced beyond the stenosis and the FCSEMS was placed over the wire (▶Fig. 2, ▶Video1). The patient was discharged the day after the procedure. The stent was removed 4 weeks later with a rat tooth forceps, and complete resolution of the stenosis could be observed (▶Video1). No adverse events were observed during the placement or removal of the stent. At 1 month followup, the patient was free of subocclusive symptoms. In conclusion, the large-bore, modified, esophageal FCSEMS can be a valid alternative in the treatment of colorectal stenosis that is nonresponsive to other endoscopic treatments.
Journal Title: Endoscopy
Year Published: 2018
Link to full text (if available)
Share on Social Media: Sign Up to like & get
recommendations!