Photo from wikipedia
Alagille syndrome (ALGS) and progressive familial intrahepatic cholestasis (PFIC) are rare, inherited cholestatic liver disorders that manifest in infants and children and are associated with impaired bile flow (ie cholestasis),… Click to show full abstract
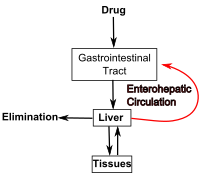
Alagille syndrome (ALGS) and progressive familial intrahepatic cholestasis (PFIC) are rare, inherited cholestatic liver disorders that manifest in infants and children and are associated with impaired bile flow (ie cholestasis), pruritus and potentially fatal liver disease. There are no effective or approved pharmacologic treatments for these diseases (standard medical treatments are supportive only), and new, noninvasive options would be valuable. Typically, bile acids undergo biliary secretion and intestinal reabsorption (ie enterohepatic circulation). However, in these diseases, disrupted secretion of bile acids leads to their accumulation in the liver, which is thought to underlie pruritus and liver‐damaging inflammation. One approach to reducing pathologic bile acid accumulation in the body is surgical biliary diversion, which interrupts the enterohepatic circulation (eg by diverting bile acids to an external stoma). These procedures can normalize serum bile acids, reduce pruritus and liver injury and improve quality of life. A novel, nonsurgical approach to interrupting the enterohepatic circulation is inhibition of the ileal bile acid transporter (IBAT), a key molecule in the enterohepatic circulation that reabsorbs bile acids from the intestine. IBAT inhibition has been shown to reduce serum bile acids and pruritus in trials of paediatric cholestatic liver diseases. This review explores the rationale of inhibition of the IBAT as a therapeutic target, describes IBAT inhibitors in development and summarizes the current data on interrupting the enterohepatic circulation as treatment for cholestatic liver diseases including ALGS and PFIC.
Journal Title: Liver International
Year Published: 2020
Link to full text (if available)
Share on Social Media: Sign Up to like & get
recommendations!