Photo from wikipedia
Address for Correspondence: Dr.Raghavendra A.Y, Associate Professor, Department of Anatomy, S.S.I.M.S & R.C, Davangere-05, Karnataka, India. Mobile-9972134242 E-Mail: [email protected] Background: Keeping in mind the frequency at which the surgical procedures… Click to show full abstract
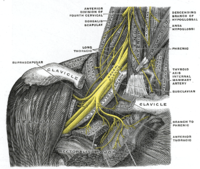
Address for Correspondence: Dr.Raghavendra A.Y, Associate Professor, Department of Anatomy, S.S.I.M.S & R.C, Davangere-05, Karnataka, India. Mobile-9972134242 E-Mail: [email protected] Background: Keeping in mind the frequency at which the surgical procedures are performed in the axilla, the organization and branching of brachial plexus and its topography becomes clinically significant and it is extremely complicated. Brachial plexus is the seat of explorations for oncosurgeons operating for breast carcinoma, schwannoma, neurofibroma, Anesthesiologists performing brachial plexus block, Plastic surgeons harboring myo-cutaneous flaps, Orthopedicians dealing with shoulder arthroplasty, humeral and clavicular fractures and for clinicians to explain the inexplicable signs of nerve compressions. The clinical importance of the variations in posterior cord is discussed in the light of various medical scenarios. Objective: To study and compare the variations in the diverse branching pattern of the posterior cord and the distance of origin of each branch in a Central Karnataka population. Materials and Methods: Branching pattern was studied by gross dissection of Brachial plexus. Origin and branching pattern and also the distance of the origin of branches of the posterior cord from mid-clavicular point on both sides were recorded. Results: UTA (L) R is the most frequent branching pattern examined in 55% of cases on right side and 60% cases on left side. Two upper subscapular nerves were found in 13% of cases on left side. Thoracodorsal nerve originated from axillary nerve on the right side in 20% cases and 15% from common trunk on left side. Lower subscapular nerve had origin from axillary nerve in 60% of cases on left side and 55% on right side. 15% of axillary nerve had origin from common trunk on left side. Radial nerve arose from the Posterior cord in 100% cases. Conclusions: Understanding the extensive array of variations involving the posterior cord and its branches, the clinicians can have a meticulous approach to axilla, respecting the facts and can utilize the facts in different cases to have a better outcome. Further study of the branching pattern of infraclavicular part of the brachial plexus is recommended.
Journal Title: International Journal of Approximate Reasoning
Year Published: 2017
Link to full text (if available)
Share on Social Media: Sign Up to like & get
recommendations!