Photo from wikipedia
An 83-year-old man was admitted to the emergency room with abdominal pain and bloating. Abdominal computed tomography (CT) revealed a sigmoid colon obstruction caused by colonic carcinoma involving a short… Click to show full abstract
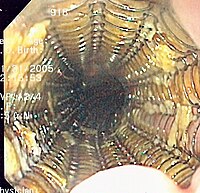
An 83-year-old man was admitted to the emergency room with abdominal pain and bloating. Abdominal computed tomography (CT) revealed a sigmoid colon obstruction caused by colonic carcinoma involving a short segment with circumferential luminal narrowing. The patient underwent endoscopy with colonic self-expanding metallic stent (SEMS) placement as a bridge to surgery. Six days after SEMS placement, the patient was prepared for esophagogastroduodenoscopy for screening. Although screening revealed no complications, 8 h later, the patient complained of sudden abdominal pain. Emergency abdominal CT revealed that the SEMS was about to burst out of the colon. An emergency operation with sigmoidectomy and colostomy was performed, and operative findings revealed a colonic perforation by the SEMS at the proximal side of the tumor. The patient was discharged from the hospital without major problems. This case is a very rare complication of colonic SEMS insertion. It is possible that increased intraluminal bowel movement and/or CO2 pressure during the esophagogastroduodenoscopy caused colonic perforation. Endoscopic placement of a SEMS is an effective alternative to surgical decompression for treating colon obstruction. To avoid unexpected and unnecessary perforations, tests that could increase the intraluminal pressure within the intestine after SEMS insertion should be avoided.
Journal Title: Revista espanola de enfermedades digestivas
Year Published: 2023
Link to full text (if available)
Share on Social Media: Sign Up to like & get
recommendations!